
What is Nephrotic Syndrome? Causes, Sign & Symptoms
Introduction:
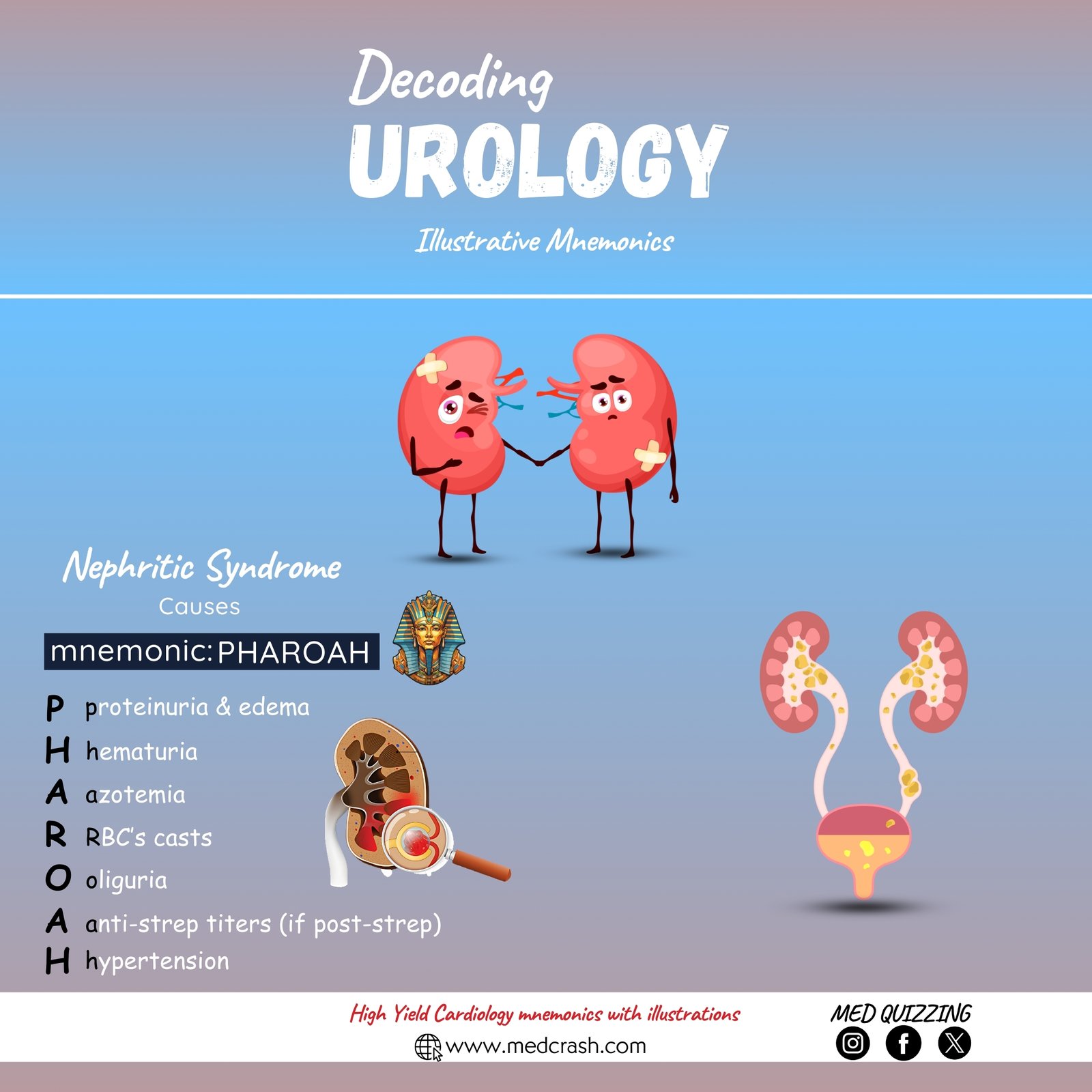
Nephrotic syndrome is defined as a set of symptoms that occur due to damage to the kidney’s filtering structure, leading to a massive leakage of proteins into the urine. This condition is characterized by significant protein loss, which disrupts normal blood protein levels.

The Nephron and Glomerulus
To understand the condition, it is essential to review the structure and function of the nephron—the kidney’s functional unit. The nephron produces urine and consists of several components, including the glomerulus, which serves as the filtering structure. The glomerulus receives fresh blood from the afferent arteriole, filtering ions, water, and waste products into Bowman’s capsule. Normally, this filtration barrier prevents proteins and red blood cells from passing into the urine. In nephrotic syndrome, however, proteins leak through the glomerulus and continue through the renal tubules, resulting in significant proteinuria.
Protein Loss and Its Consequences
Patients with severe nephrotic syndrome can lose three grams or more of protein per day. This massive proteinuria leads to a decrease in essential proteins that should remain in the bloodstream, causing various complications. One of the most critical proteins lost is albumin.
Albumin and Oncotic Pressure
Albumin plays a vital role in regulating oncotic pressure in the blood. When albumin is lost in large amounts, blood albumin levels drop, leading to hypoalbuminemia. As a result, the body loses its ability to regulate oncotic pressure effectively, and fluid begins to leak into the interstitial spaces, causing significant edema.
Mechanism of Edema and Hyperlipidemia
A decrease in albumin causes water to escape from the capillaries into the surrounding tissues, resulting in widespread swelling. Additionally, low albumin levels prompt the liver to produce more albumin. However, this process also increases the synthesis of cholesterol and triglycerides, leading to hyperlipidemia. This scenario is particularly concerning in pediatric patients, where high cholesterol levels can be a red flag.
Additional Protein Loss and Infection Risk
In nephrotic syndrome, patients also lose immunoglobulins—proteins that play a crucial role in fighting infections. The loss of these proteins increases the patient’s susceptibility to infections. Furthermore, treatments such as corticosteroids, which suppress the immune system, add to the risk.
")
Risk of Clot Formation
The condition also leads to the loss of proteins that normally help prevent blood clot formation. Without these proteins, patients are at an increased risk for developing blood clots, such as deep vein thrombosis or pulmonary embolism. It is important for healthcare providers to monitor for these complications.
Causes of Nephrotic Syndrome
Nephrotic syndrome is not a single disease but a set of symptoms that can result from various underlying causes. The causes can be classified into primary and secondary categories:
Primary Causes:
These are associated with intrinsic kidney problems. Minimal change disease is the most common cause in pediatric patients aged 2 to 5, detectable only by an electron microscope. Other primary causes include focal segmental glomerulosclerosis and membranoproliferative glomerulonephritis.
Secondary Causes:
These occur when other systemic diseases damage the kidney’s glomeruli. Conditions such as lupus, diabetes, hepatitis, heart failure, HIV, and the use of medications like NSAIDs can lead to nephrotic syndrome. Patients may experience periods of remission followed by relapse, making ongoing education and monitoring essential.
")
Signs and Symptoms of Nephrotic Syndrome
Key signs and symptoms include:
- Massive Proteinuria: Loss of three grams or more of protein per day, resulting in foamy or frothy urine.
- Hypoalbuminemia: Low blood albumin levels that lead to edema.
- Edema: Swelling typically begins in the face and around the eyes, progressing to the extremities and abdomen as the condition worsens.
- Hyperlipidemia: Elevated cholesterol and triglyceride levels due to compensatory liver activity.
- Increased Risk of Infection: Loss of immunoglobulins predisposes patients to infections.
- Risk of Clot Formation: Increased likelihood of blood clots due to the loss of protective proteins.
Management
Fluid Management:
Monitor fluid status with daily weights and strict intake and output measurements. Diuretics may be used to reduce fluid overload, and IV albumin may be administered if needed. Pediatric patients should maintain an output of at least 1 mL per hour per kilogram, and adults should have at least 30 cc’s per hour.
Edema and Skin Care:
Regularly assess swelling, especially in the abdomen and extremities. Monitor for skin breakdown, and ensure that patients wear loose clothing and use sensitive tapes to prevent skin injury.
Infection Prevention:
Meticulous handwashing, monitoring temperature, and educating families about the signs of infection are crucial, especially for patients on corticosteroids or immunosuppressants.
Clot Prevention:
Keep a close watch on respiratory status, heart rate, and signs of chest pain to identify potential pulmonary embolism or deep vein thrombosis early.
Dietary Management:
Implement a low sodium and low-fat diet as prescribed to manage fluid retention and hyperlipidemia.
Patient Education:
Educate patients and their families about the importance of monitoring proteinuria, recognizing signs of relapse, and understanding the risks of infection and clot formation.